
Paediatric aortic valve replacement using decellularized allografts: A multi-centre update following 143 implantations and 5-year mean follow-up
Samir Sarikouch MD, PhD
Hannover Medical School, Department of Cardiothoracic Surgery, Hannover, Germany
Options for pediatric aortic valve replacement (AVR) are sparse once aortic valve repair is not feasible. Decellularized aortic homografts (DAH) may constitute an additional AVR option in children as they hold the potential to overcome the high early failure rate of conventional allogenic and xenogenic aortic valve prostheses while avoiding the inherent risks of mechanical prostheses associated with anticoagulation.
143 decellularized aortic homografts (DAH) were implanted between 2/2008 and 2/2023 in 137 children (106 male, 74 %) with a median age of 10.8 years (IQR 6.6-14.6, mean 10.4 ± 4.8 years). Follow-up was complete. 84 (59 %) had undergone previous cardiac operations (47 with 1, 24 with 2, 13 with ³ 3 previous operations). 24 (17 %) had undergone previous AVR (19 with 1, 4 with 2, and 1 with 3 previous operations). The median implanted DAH diameter was 21 mm (IQR 19-23). The median operation duration was 348 min (IQR 227-439) with a median CPB time of 212 min (IQR 171-257) and a median cross-clamp time of 135 min (IQR 113-164).
After a median follow-up of 5.3 yrs. (IQR 3.3-7.2, max. 15.2 yrs.), the primary efficacy endpoints peak gradient of median 14 mmHg (IQR 9-28) and regurgitation of median 0.5 (IQR 0-1, Grade 0-3) showed good results but an increased progression over time.
Freedom from death was 97.8 and 96.3 % at 5 and 10 years, an outstanding result, which underlines the expertise of the participating centres. Adverse events such as re-operation, valve degeneration, endocarditis or thromboembolism after a median follow-up of 5.3 years were comparable to the results from current paediatric Ross cohorts, despite patients undergoing twice as many previous cardiac operations (59 vs. 32.3 %) and significantly more previous AVR (17 vs. 2.3 %). The medium to long-term results, however, also demonstrate rising gradients and regurgitation in DAH over time leading to surgical re-intervention. Despite thorough decellularization and detailed quality assurance through individual DAH testing before release, DAH appear to elicit a low-grade immune response, which, in contrast to classic T-cell mediated immune reactions, is thought to be more antibody-mediated.
Figure 1 exhibits the patient with the longest follow-up after redo DAH implantation.
Following two balloon dilatations, he underwent AVR with a 10 mm DAH at the age of 2 months in 2010 and a subsequent re-do AVR in 2015 with a 17 mm DAH due to subvalvular stenosis leading to aortic regurgitation by Jet-lesion destruction of one cusp. The patient had normal left ventricular and homograft function 8 years after the redo procedure.
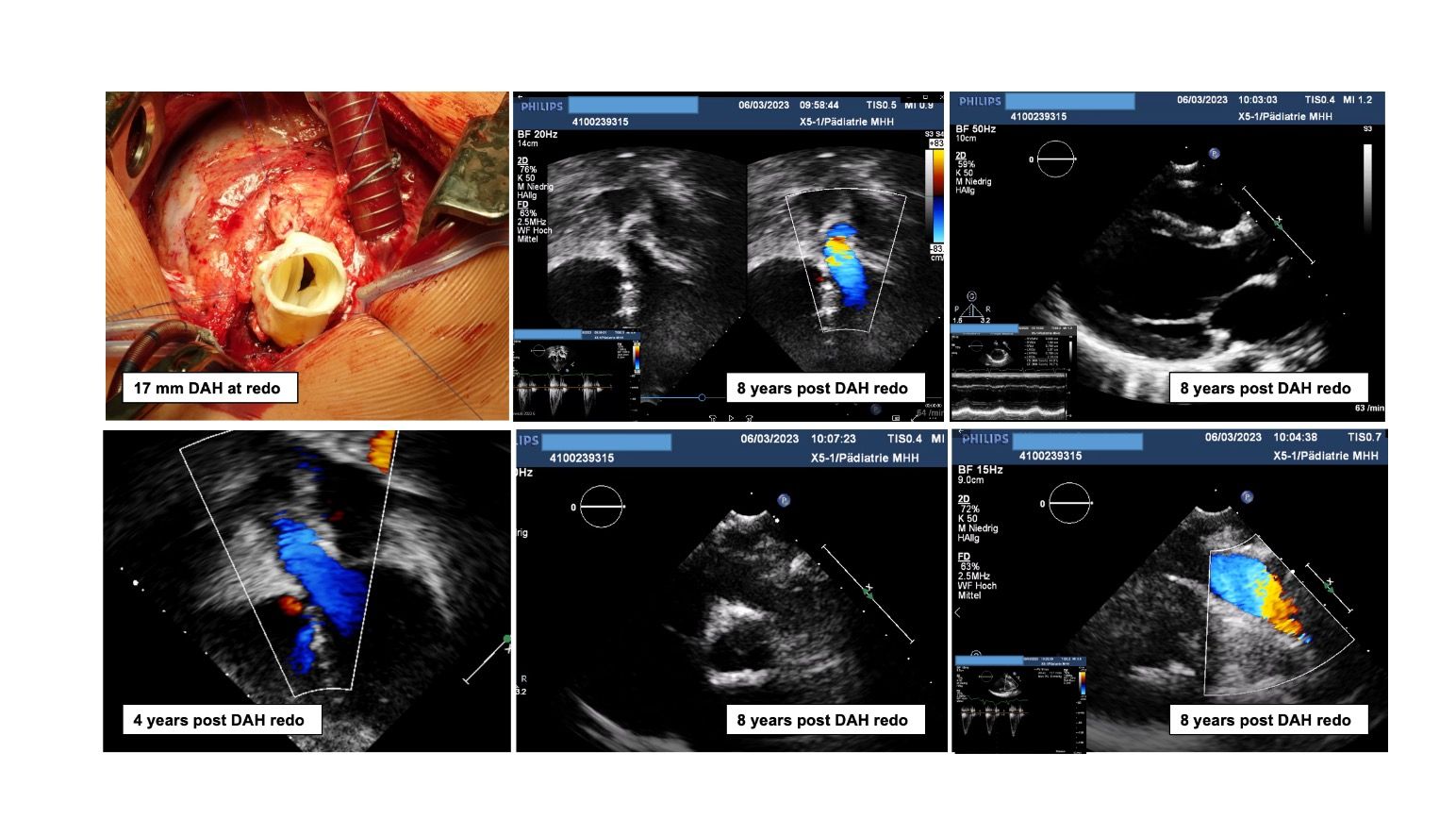
Figure 1 - 0.2-year old boy, S/P 2 x aortic valve balloon valvuloplasty, AVR with DAH 10 mm in 2010 and re-do AVR in 2015 with 17 mm DAH. Recent echocardiography 8 years after re-do DAH implantation shows normal ventricular dimensions and function. Competent and pliable DAH cusps and a normal, untouched pulmonary valve. DAH- decellularized aortic homograft, AVR – aortic valve replacement